Table of Contents
PCOS vs PCOD – What’s the Difference? A Comprehensive Clinical Overview
In the realm of women’s reproductive health, the terms PCOD (Polycystic Ovarian Disease) and PCOS (Polycystic Ovary Syndrome) are frequently used interchangeably. However, from a clinical perspective, they represent two distinct levels of hormonal and metabolic dysfunction. While both conditions involve the ovaries and can impact a woman’s menstrual cycle, their implications for long-term health, fertility, and systemic wellness differ significantly.
Understanding these nuances is essential for any woman navigating irregular cycles or hormonal symptoms. PCOD is generally considered a functional imbalance, often manageable through lifestyle shifts, whereas PCOS is a complex endocrine system disorder with broader metabolic consequences. This guide provides a scientifically grounded breakdown of PCOS vs PCOD, helping you identify the specific characteristics of each and the clinical pathways required for effective management.
Overview of PCOD and PCOS
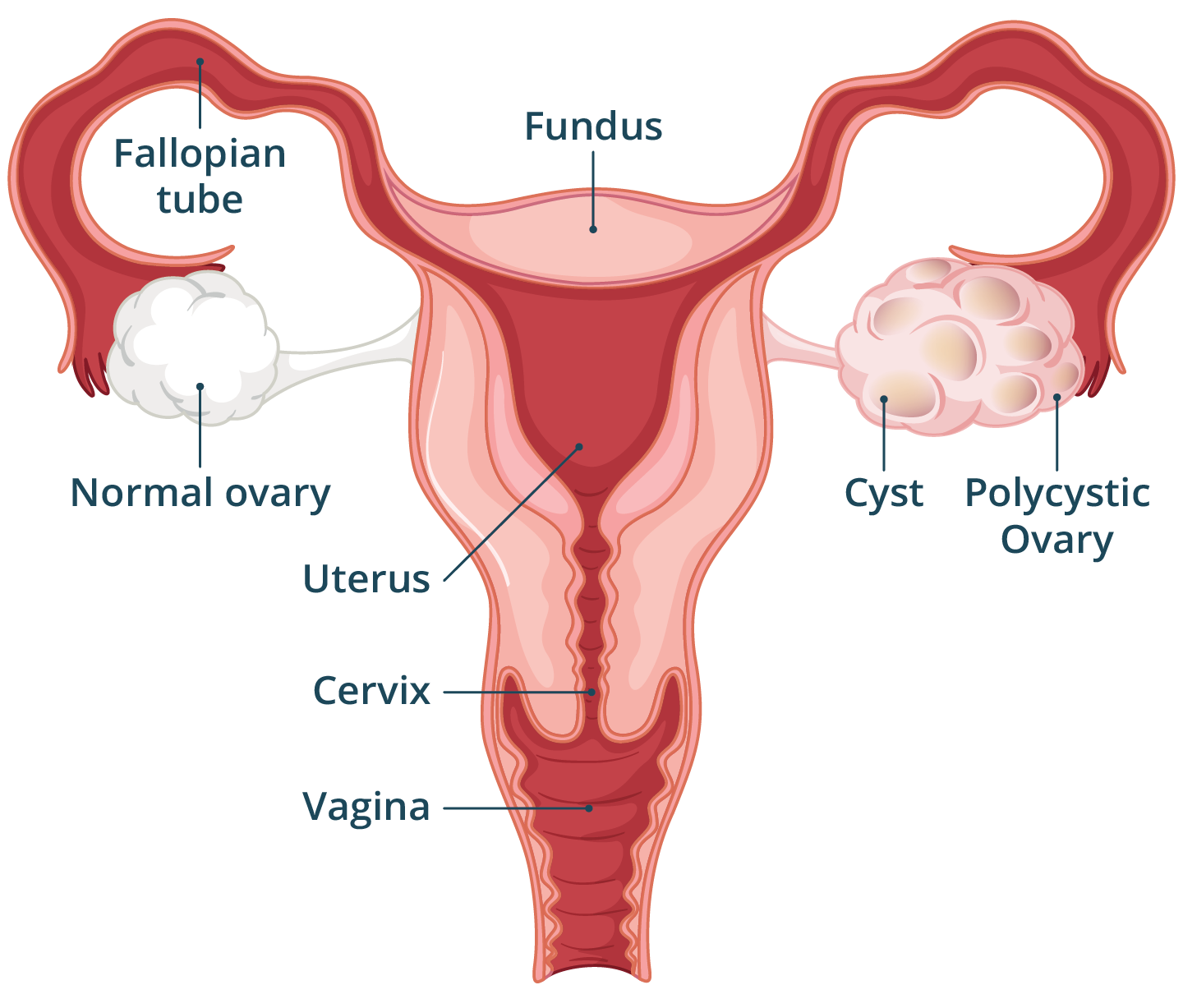
What is the difference between PCOD and PCOS? The primary distinction lies in the severity and the systems involved. PCOD (Polycystic Ovarian Disease) is a condition where the ovaries produce immature or partially mature eggs due to poor lifestyle, stress, or hormonal fluctuations, which eventually turn into cysts. It is often considered a common condition that may not significantly impact fertility in the long run.
In contrast, PCOS (Polycystic Ovary Syndrome) is a metabolic and endocrine disorder. In PCOS, the ovaries produce excessive amounts of androgens (male hormones), which interfere with the development and release of eggs. PCOS is a more severe condition that can lead to systemic issues like insulin resistance, Type 2 diabetes, and cardiovascular complications.

Comparative Analysis: Causes, Symptoms, and Biology
1. The Biological Root
- PCOD: Often triggered by an imbalance in the ratio of hormones, frequently linked to a sedentary lifestyle, high-stress levels, or poor nutritional habits. The ovaries usually remain functional but release immature eggs that attach to the ovarian walls.
- PCOS: Rooted in the endocrine system. It involves a significant overproduction of testosterone and a high degree of insulin resistance. It is often linked to genetic predispositions and low-grade chronic inflammation.
2. Symptom Presentation
While both share symptoms like irregular periods, the intensity varies:
- PCOD Symptoms: Irregular menstrual cycles, occasional weight gain, and mild acne. Many women with PCOD do not experience significant hair loss or excessive facial hair.
- PCOS Symptoms: Severe acne, hirsutism (excessive facial and body hair), male-pattern baldness, significant difficulty losing weight, and darkened skin patches (acanthosis nigricans).
3. Impact on Fertility
- PCOD: Women with PCOD can often conceive with minimal medical intervention. The ovaries still function relatively well, and lifestyle corrections often restore regular ovulation.
- PCOS: Infertility is a more common challenge due to chronic anovulation (lack of egg release). Conceiving often requires specialized medical support to induce ovulation.
Key Insights and Practical Guidance
Differentiating these conditions requires a structured diagnostic approach involving blood work and imaging.
- Diagnostic Markers: A gynaecologist will typically look for the “Rotterdam Criteria” for PCOS, which includes irregular periods, high androgen levels in blood tests, and the “string of pearls” appearance of follicles on a pelvic ultrasound.
- Lifestyle as Medicine: For PCOD, the first line of defense is a regulated diet and consistent exercise. For PCOS, lifestyle changes are mandatory but are often supplemented with medications like Metformin (for insulin) or hormonal regulators.
- Metabolic Monitoring: Women with PCOS should regularly monitor their HbA1c and lipid profiles, as they are at a higher risk for metabolic syndrome compared to those with PCOD.
When to Seek Medical Help
Early clinical intervention can prevent the progression of PCOD into more severe metabolic stages. You should consult a specialist if:
- Your menstrual cycles are consistently longer than 35 days.
- You notice sudden, rapid hair growth on your face, chest, or abdomen.
- You are struggling to conceive after 12 months of unprotected intercourse.
- You experience persistent adult acne that does not respond to dermatological treatments.
- You have a family history of diabetes and are experiencing irregular cycles.
3. Visakhapatnam Section
People in Visakhapatnam seeking women’s healthcare often consult qualified specialists to differentiate between these conditions. Clinics in areas such as Madhurawada, MVP Colony, and Dwaraka Nagar provide access to advanced ultrasound diagnostics and hormonal assays. Facilities like Vedanta Speciality Clinics are among those offering structured care for such conditions, providing residents of the Vizag region with evidence-based management plans for both PCOD and PCOS.
4. FAQ SECTION
Is PCOS more dangerous than PCOD?
PCOS is generally considered more serious because it is a metabolic disorder. While PCOD primarily affects the ovaries and menstrual regularity, PCOS can lead to long-term health complications such as Type 2 diabetes, high blood pressure, and increased risk of endometrial cancer if left unmanaged for years.
Can PCOD turn into PCOS over time?
PCOD does not “turn into” PCOS, but an unmanaged lifestyle in a woman with PCOD can worsen hormonal imbalances and insulin resistance, leading to more severe symptoms. If the metabolic markers (like insulin levels) become significantly disrupted, the condition may then meet the diagnostic criteria for PCOS.
Which is more common, PCOD or PCOS?
PCOD is more common than PCOS. It is estimated that a large percentage of women globally have some form of PCOD, often manageable through diet and exercise. PCOS is less common but still affects roughly 10% of women of reproductive age worldwide.
Can I get pregnant naturally with PCOS?
Yes, natural conception is possible with PCOS, but it is more challenging than with PCOD. Many women with PCOS require medical assistance to stimulate ovulation. However, with proper weight management and hormonal balancing, many are able to conceive naturally or with minimal clinical help.
Do all women with PCOS have cysts on their ovaries?
Surprisingly, no. Despite the name, you do not need to have “cysts” (follicles) to be diagnosed with PCOS. According to the Rotterdam Criteria, if you have irregular periods and high androgen levels, you can be diagnosed with PCOS even if your ultrasound appears normal.
Is weight loss more difficult with PCOS or PCOD?
Weight loss is typically much more difficult with PCOS. This is because PCOS is closely linked with insulin resistance, which causes the body to store fat more easily and makes it harder for the body to use stored energy. PCOD weight gain is usually easier to manage.
5. CONCLUSION
In summary, while PCOD and PCOS share a common name, they represent different levels of health challenges. PCOD is often a manageable hurdle through disciplined lifestyle choices, whereas PCOS requires a comprehensive medical and metabolic strategy. Regardless of the diagnosis, early detection and consistent monitoring are the keys to maintaining reproductive health. Seeking guidance from an experienced women’s healthcare specialist can help ensure proper diagnosis and personalized care.



Leave a Comment